Every Friday you get the latest from the world of Emergency Medicine:
Literature Reviews, ECG Challenges, Podcasts, Mini-lectures and more.
“The Knowledge You Take To Your Next Patient DOES Matter”
Every Friday you get the latest from the world of Emergency Medicine:
Literature Reviews, ECG Challenges, Podcasts, Mini-lectures and more.
“The Knowledge You Take To Your Next Patient DOES Matter”

⚡ Clinical Takeaways
Below is a section of the writeup on the resus blog.
The Eastern Society for the Surgery of Trauma (11) in their approach to screening suspected BCI patients, did not consider isolated sternal fractures to predict BCI. They also proposed no further investigations in patients with a normal ECG and Troponin If all else was normal, the recommendation was for no monitoring of these patients.
This is where it becomes a little harder. There is a move away from working up isolated sternal fractures, however the evidence (some of which is presented below) is not robust. Due to this reason, my approach is to perform an ECG and high sensitivity troponin on patients with suspected BCI due to mechanism and clinical presentation. These are simple and inexpensive tests that can give us a lot of information. They aren’t perfect however and can be associated with false positives and negatives.
When should we investigate the patient with suspected blunt cardiac injury (BCI) and how do we work them up?
The evidence is mostly made up of retrospective studies and case studies.
The main areas of uncertainty involve:
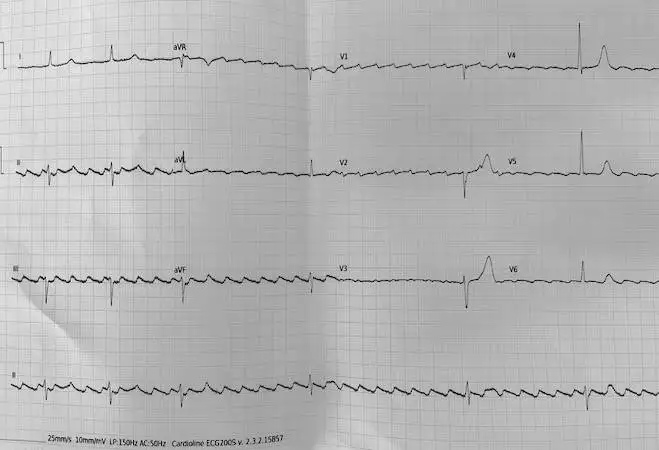
A 78yo male woke up in the morning feeling dizzy. The patient was well when lying down, but became light headed every time he got up. He waited, but symptoms did not improve, so later in the afternoon he attended the Care Centre. Not all the past history is available, but there is a history of CAGS and atrial fibrillation/flutter for which he was on Diltiazem. The patient was alert and well and there was no chest pain or SOB. The blood pressure was 130/80 and the heart rate was… as you see below. What does the ECG show? What is the diagnosis and what do you do now?

The Efficacy of targetting high MAP for older patients with Septic Shock
Should we be targeting a higher MAP in that subset of patients with sepsis who progress to shock? Mortality is high in the elderly and even higher in the very old.
What They Did
This was a multicentre, pragmatic, open-label, randomised controlled trial at 29 Japanese centres, randomising patients >65 years old with septic shock.
Patients were randomised to a higher blood pressure group (MAP = 80-85 mmHg) or a control group (65-70 mm Hg). The target MAP was maintained for 72 hours or until pressors were no longer needed.
If a noradrenaline dose of at least 0.1mcg/kg/min was required to maintain the MAP, Vasopressin was commenced and could be increased to 0.04 U/min.
Primary Outcome: All cause mortality at 90 days.
What They Found…..
Outcomes
Targeting a higher MAP of 80–85 mmHg significantly increased mortality compared with targeting a MAP of 65–70 mmHg.
Read the whole study on the ResusBlog.
Do we need arterial lines in shock?
Is managing shock without early arterial catheterization, noninferior to early catheter insertion with regard to death from any cause at 28 days?
What They Did
This was an open-label, investigator-initiated, pragmatic, multicenter, parallel-group, noninferiority, randomized, controlled trial, conducted in 9 ICUs in France. n=1010
What They Found
With respect to mortality by day 28, delaying arterial catheterisation and using NIBP was non-inferior to arterial catheterisation. This avoided arterial catheterisation in 85% of patients.
My Take on This
This is an unblinded trial and found that non-invasive blood pressure monitoring was not inferior to invasive blood pressure monitoring in shock. If we look a little more closely we see the following that this study predominantly looked at septic shock………
Will this paper change our practice? Should it? Read my whole take on this on the ResusBlog.


