
EMCORE Newsletter 29/11/23
This week’s we look at:
- EMCORE Queensland: We’ve made a further 5 places available. It’s going to have fun! Book Now.
- 4 Cases of Shocked Patients: Which Inotrope/Pressor to use? Is there one that suits every situation? I take you through the choice of drugs to maximise resuscitation of your patients.
- STEMI Equivalents: do you know what they are? Read the summary from the 2022 guidelines.
- A Patient with Propranolol overdose. How would you treat this? This was a real case, that had us throwing everything plus the kitchen sink at the patient. It scared us all. Read about it.
- The new EMCOURSE learning platform will be announced in 2 weeks. This is all your learning and CPD points in one place. I am so excited about this!
- EMCORE London and Fiji will be incredible. Program up next week. Seats filling now.
THE SHOCKED PATIENT: WHICH INOTROPE OR PRESSOR TO USE
4 Cases of Shocked patients. Which pressors/inotropes would you use?
CASE 1: Urosepsis with the following vitals: T 38.9, HR 115bpm, BP 65/42, Sats 96% on room air.
The patient has received two litres of crystalloid with no change in BP. What do you give next?
CASE 2: Sepsis with a history of atrial fibrillation, on Sotalol. The patient has the following vitals: T 38.9, HR 28bpm, BP 68/40, Sats 96% on room air. Acute renal failure is suspected as the VBG shows a potassium of 7.8mmol/l. What inotrope(s) and/or pressor(s) will you use here?
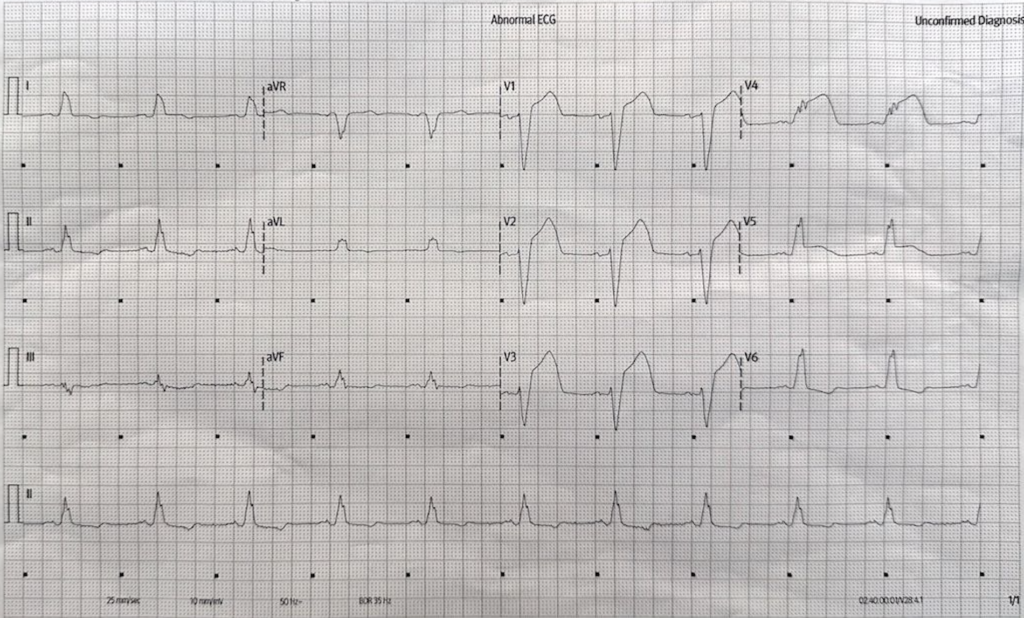
CASE 3: A 65 yo male with 3 hours of chest pain, in cardiogenic shock, with acute pulmonary oedema. The ecg shows STE in aVR and widespread ST depression. Vitals are: T 36.7, HR 104bpm, BP is 71/50, Sats of 90% on 10L/min oxygen. How will you support the blood pressure here?
CASE 4: A patient is diagnosed with a pulmonary Embolism on CTPA. On returning from the CTPA the vitals are: T 37.1, HR 132bpm, BP 68/36, Sats 88% on 6 L/min O2 . How would you treat this patient’s blood pressure now?
Go to the RESUS BLOG to read the solution to these cases and a short review of all pressors and inotropes that are relevant and listen to the 15 minute podcast.
STEMI EQUIVALENTS: ONLY 4 TO REMEMBER
These ECG criteria identify patients who require immediate reperfusion therapy as per the 2013 STEMI Guidelines. The ecg changes may not show ST elevation, however these changes have been associated with coronary artery occlusion and we must know them.
Read it on ECG of the Week
A PATIENT WITH PROPRANOLOL OVERDOSE: ONE FROM THE VAULT
A 26 yo woman is brought to the ED by ambulance. She has been found by her mother in a confused state. The ambulance report that there are 60 x 40mg tablets of Propranolol that are missing.
On arrival the patient’s GCS is 9 and vitals are: HR 60 bpm, BP 105/40 mmHg, Sats 98% on 6L/min O2, RR 20 breaths per minute. Within 5 minutes of arrival the patient has a generalised tonic clonic seizure lasting less than 30 seconds. Soon after the heart rate drops to 45bpm and the BP to 80/50.
This is based on a real case…. a case we might all get and an important one for the Fellowship Candidates to read.
How toxic is propranolol overdose? What is considered a lethal dose?
What are the ECG changes seen. How would you treat this overdose?
A QUICK ANNOUNCEMENT
I’ve spoken about the EMCOURSE on the new Learning Platform EMMastery. It’s coming in 2 weeks. Membership is free for free stuff, and if you invest the price of 1-2 cups of coffee per week, you get a total learning platform and CPD, which will include:
The EMSHOW: Podcasts and discussions recorded for you to listen to later
EM Lectures: A short Emergency Medicine Syllabus
Lit reviews: A monthly roundup of the most important Resus, Cardiac, Trauma, and Paeds papers
Cardiac Bootcamp: The total course included in the price.
Fellowship Flurry: Not only of registrars but for everybody: Super knowledge at Exam Level + Quizes
Grand Rounds: Monthly Live webinar lectures and Discussions on major Clinical Topics/Controversies.
…….. and MORE. Going Live in 2 weeks.
Listen to the podcast on APPLE PODCASTS and SPOTIFY.
SEE YOU AT EMCORE
I am looking forward to these conferences in 2024. Join us for what will be AMAZING experiences, with superstar speakers and state of the art topics!



That’s all I’ve got for you this week. Enjoy and see you soon at EMCORE
Peter Kas
JOIN US FOR A COURSE