
EMCORE Newsletter 7/12/23
This week:
- EMCORE Queensland: Registration closing soon. If you haven’t booked the new Cardiac Bootcamp yet, Book Now. See you there.
- The Case of a dizzy patient in Atrial Flutter with an 8:1 Block. How would you treat this? Watch the video for a discussion of flutter and medications.
- Beware the patient with sudden onset of headache and normal CT. Know the mimics.
- Recently I posted the case of the child that wouldn’t stop seizing. This week we have a new paper published on Nonconvulsive Status Epilepticus for Emergency Physicians that we review.
- Levetiracetam associated with severe life threatening reaction (DRESS).
ATRIAL FLUTTER WITH A HIGH DEGREE BLOCK
A 78yo male woke up in the morning feeling dizzy. The patient was well when lying down, but became light headed every time he got up. He waited, but symptoms did not improve, so later in the afternoon he attended the Care Centre. Not all the past history is available, but there is a history of CAGS and atrial fibrillation/flutter for which he was on Diltiazem. The patient was alert and well and there was no chest pain or SOB. The blood pressure was 130/80 and the heart rate was… as you see below. What does the ECG show? What is the diagnosis and what do you do now?
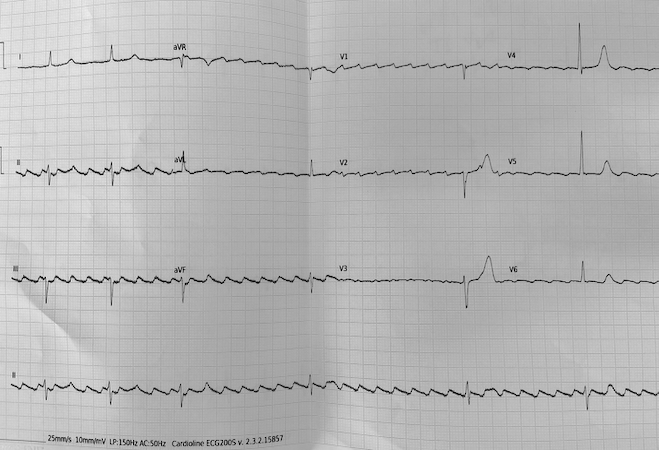
Watch the Video discussion and read the summary on the Resus Blog
NONCONVULSIVE STATUS EPILEPTICUS
There is no consensus agreement on diagnostic criteria, or management. It may be that an electroencephalogram (EEG), is a main way to make the diagnosis. However this is not 100% specific and rarely available in the emergency department.
What we know is that NCSE is associated with an overall poor prognosis, with the most important determinant of mortality and morbidity being the cause of the seizure. The longer the duration of NCSE, the greater the mortality. This is not related to respiratory failure or lactic acidosis or rhabdomyolysis as occurs in convulsive status, but more due to sustained neuronal excitation.
Abnormal ocular movements, which include, blinking, twitching of the eyelids, pupillary dilatation, gaze deviation or nystagmus have a greater than 80% specificity of NCSE.
A PATIENT WITH SUDDEN ONSET OF HEADACHE AND NORMAL CT. ARE WE DONE?
KNOW THE MIMICS
You’ve just seen a patient with sudden onset of headache. They have presented within 6 hours and your super-sliced scanner spits out a normal CT brain. Are you done? You apply shared decision making with your patient and decide against a lumbar puncture. Are you done? Beware the mimics; amongst them cerebral venous thrombosis and carotid artery dissection.
Read the clinical summary here.
UPDATE: LEVETIRACETAM ASSOCIATED WITH LIFE THREATENING REACTIONS
DRESS (Drug reaction with eosinophilia and systemic symptoms), is being seen in very small numbers in patients on levetiracetam. It’s a severe drug reaction which involves:
- Skin Rash that is extensive
- Organ involvement and failure
- Lymphadenopathy
- Eosinophilia and
- Atypical Lymphocytosis.
It is rare and doesn’t occur following a dose being given in the emergency department. It appears 2-8 weeks following commencing Levetiracetam. We need to be aware of this rare reaction as it mimics Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis, which are also rare
SEE YOU AT EMCORE
I am looking forward to these conferences in 2024. Join us for what will be AMAZING experiences, with superstar speakers and state of the art topics!



That’s all I’ve got for you this week. Enjoy and see you soon at EMCORE
Peter Kas
JOIN US FOR A COURSE